As part of the Maa Hub-spokes (HS) model, specialised doctors will be working in the Maa clinic to deliver comprehensive antenatal care to high-risk mothers. This report outlines the purpose of the Maa clinic and the responsibilities of the specialised doctors.
As part of the Maa Hub-spokes (HS) model, specialised doctors will be working in the Maa clinic to deliver comprehensive antenatal care to high-risk mothers. This report outlines the purpose of the Maa clinic and the responsibilities of the specialised doctors. It will also explore the evidence-base behind establishing this role within the HS model, highlighting how Maa will be adopting and improving elements of similar programmes that have been implemented.
The Maa clinic and Specialised Doctors
The primary role of the Maa clinic is to act as a ‘Hub’ in the Hub-spokes model. The Maa clinic is set up inside a government-owned Upazilla Health Complex in Moulvibazar (district-level health clinic). This ensures the clinic is easily accessible to mothers, as the distance between the clinic and their homes is short.
Maa’s specialised doctors are foundation year doctors in Bangladesh, who will receive an intensive 6-month training course on maternal healthcare, designed by RCOG BD. Upon completion of this training course, doctors will receive a certificate from RCOG UK. As part of the training programme, doctors must complete a 3-month rotation at the Maa clinic. Failure to complete this rotation will result in loss of the qualification, hence Maa is ensuring that doctor absenteeism is not an issue in the HS model (discussed in detail below). The programme has been designed to ensure that there are always two Maa doctors working 9am-5pm shifts and one Maa doctor will be available on-call. Doctors will rotate every three months with some overlap to ensure proper handover of cases.
The doctors’ role in the HS model is equivalent to a GP in the UK. They will provide advanced ANC to high-risk mothers identified by Maa’s Health Brigade Members (HBMs), and diagnose and manage red flag symptoms and other non-communicable diseases which increase the risk of a poor pregnancy outcome. Maa doctors are the only healthcare workers in the HS model who are qualified to prescribe medication to mothers. This is necessary because problems such as hypertension can be managed by medication and subsequently prevent or at least reduce the risk of a complicated birth. Similarly, doctors will be able to administer drugs such as Misoprostol to prevent post-partum haemorrhages, the leading cause of maternal death worldwide (WHO, 2012).
Mothers will be given either weekly or fortnightly appointments to ensure they are continuously monitored for complications. In case of complications, doctors are responsible for rapid referral to the local district hospital, and transport will be arranged for those families who have difficulty. We hypothesise that the doctors will help reduce maternal mortality and morbidity in the target population by ensuring mothers receive care in a timely manner.
The Importance of primary healthcare practitioners in maternal healthcare
United Kingdom
The role of a General Practitioner (GP) in the UK is to provide primary healthcare (PHC) services. PHC is a community-based, preventative approach to healthcare. GPs are expected to recognise and manage a person’s health needs, which can be physical, social or psychological in nature. Their aim is to prevent life-threateningconditions and provide treatment (WHO, 2019). In high-income countries, like the UK, GPs are the first point of contact for pregnant women, despite the availability of self-referral systems to a midwife. Studies have shown that the overall role of GPs in pregnancy has declined in the UK over the past decade. This is mainly due to changes in policies. Research by the King’s Fund (2010) explored the role of GPs in maternal healthcare. They found that, although policies were encouraging the use of midwives, there are rural areas in the UK where midwifery services are not abundant. Thus, GPs are required to manage maternal healthcare; similar to the situation in low- and middle-income countries (LMICs). The King’s Fund report suggests a number of potential roles for GPs before, during and after pregnancy. For example, providing telephone consultations for mothers who live in remote areas and urgent referrals to secondary and tertiary care units in hospitals.
Low- & Middle-Income Countries
Interestingly, LMICs like Bangladesh do not currently have a strong midwifery-led programme, despite growing evidence of its potential. Therefore, there is a gap in the provision of maternal healthcare in the PHC setting. This emphasizes the importance of Maa’s specialised doctors to provide the required care to mothers and babies. Unlike the UK, a major barrier to reducing maternal mortality in LMICs is the absence of a strong, reliable referral system between primary, secondary and tertiary healthcare facilities. This endangers women, particularly those in hard to reach, suburban and rural areas.
Pembe and colleagues (2010) show that in the Rufiji District of Tanzania, 28% of pregnant women were referred to the district hospital. The majority (70%) of these referrals were due to demographic risk factors such as being less than 20 years of age or having had more than 5 pregnancies in the past. Rapid referral allowed mothers to get appropriate care when required. Only 4 out of the 643 mothers who were referred died in the hospital. Despite this success, a key observation in this study was a lack of compliance when mothers were referred or advised to go to a hospital by a healthcare provider after an ANC in the clinic. Less than half of the women acted on this advice and sought follow-up care at the hospital, and the major reasons for non-compliance were financial constraints and difficulty arranging transport. The HS model will provide continuous encouragement and education to women and their families regarding maternal health and risks during pregnancy via HBMs and Women’s Groups (WGs). We hypothesise that this will reduce the rate of non-compliance in our study. WGs will also teach and encourage mothers and families to budget for a situation in which sudden complications may arise and they are required to pay hospital fees and transportation costs.
Conversely, another important issue raised in this paper is that if too many referrals are made, this can overburden the district hospital with normal deliveries, leading to improper, low-quality emergency obstetric care. To avoid this situation, the HS model ensures mothers will be followed up frequently during their pregnancy for ANC by both HBMs (low-risk) and doctors (high-risk), in order to have a very clear idea of which mothers really need tertiary care and for whom management of symptoms using medication will be enough to have a normal delivery at home or in a local clinic facility.
A study published in 2018, investigated the effectiveness of actions taken by PHC professionals in rural areas of Brazil (Figueirdo et. al., 2018). The main conclusion of this study was that in order to reduce maternal mortality, they must work as a team. This team is usually comprised of physicians, physical educators of pregnancy and maternal health, and psychologists. The most useful PHC interventions in reducing maternal mortality were home visits, education sessions, prenatal care consultations and active searches for pregnant women. The HS model has taken all of this into account, to form a well-structured PHC system in Moulvibazar. Maa WGs will educate and empower women, and identify newly pregnant mothers. These mothers will then be added to the database by HBMs and have ANC check-ups at home. If they are suspected to be at high risk, HBMs will refer them to the Maa clinic, where qualified graduate physicians (Maa specialised doctors), will have consultations. These consultations will be equivalent to GP consultations in the UK, whereby mothers will have advanced ANC and their symptoms will be managed using prescribed medicines. Mothers will be told to attend further consultations, should the doctor feel it necessary. Here, they will also be told about the importance of postnatal care and encouraged to attend the clinic. This allows continuity of care during the entire critical period of the pregnancy.
Achieving social equity in maternal healthcare
de Jonge et al. (2018) discuss an extremely important issue in the context of equity and place of birth. As discussed above, clinic births are safer for both mother and child, however, from 2005 to 2009, only 17% of births in Bogra, Moulvibazaar and Faridpur took place at a healthcare facility (de Jonge et. al., 2018). An important reason for such a low percentage is that women of lower socioeconomic status could not access a clinic facility as easily as women of higher socioeconomic status. Interestingly, this report suggests that of those illiterate women who did manage to attend a clinic facility, the majority received poorer quality of care by comparison to literate women. The authors suggest that this difference may be due to two reasons: literate mothers actively seek a better quality of care for themselves and their baby, and there is an inherent bias in health workers’ behaviour i.e. they are prejudiced towards illiterate women, hence introducing inequality in the standard of care provided. The Maa clinic will begin to break this norm of social inequality in healthcare, by providing easy access to a healthcare facility (at least in terms of location) to a population of mothers who are otherwise missing out on the benefits of facility births. This will be via rapid referral of high-risk mothers to a local government hospital. Based on this research, it is imperative that the Maa Bangladesh team ensure that any prejudiced behaviours by Maa healthcare workers are immediately flagged and appropriate actions are taken to prevent this becoming an issue in the Maa clinic. One way Maa aims to achieve this is by exploring and unlearning this unconscious bias during training at all levels of our HS model.
Surgical task shifting
A vast shortage of specialised doctors in rural areas of developing countries is responsible for high maternal mortality and morbidity rates, as mothers are unable to access emergency care. Some developing countries have adopted the idea of ‘task shifting’. Task shifting involves training mid-level doctors, such as foundation level doctors, to be able to perform basic procedures in emergency settings, without the need for a consultant to be present. In the past, several studies have evaluated the effectiveness of task shifting in West African countries.
Recently, the Ministry of Health and Sanitation in Sierra Leone and the NGO called CapaCare, initiated a surgical task shifting training programme (van Duinen et. al., 2019). This programme trained ‘Associate Clinicians’ (AC) to deal with basic emergency surgical and obstetric problems, including C-sections. ACs included junior doctors, but more interestingly, community health workers who had more than 2 years of work experience were also enrolled inthe programme. The main finding of this study indicates that C-sections carried out by ACs did not lead to a higher maternal mortality rate, by comparison to consultants.
Interestingly, Mali has been dependent on ‘Clinical Officers’ (COs) for providing healthcare, including advanced EmOC, in rural areas (Chilopora et. al., 2017). COs are mid-level, non-doctor, healthcare providers, who receive intensive training for a year at central or district-level hospitals. The study revealed that COs performed 88% of all emergency care operations in district-level hospitals. When factors such as mortality, maternal outcome and neonatal outcome were compared between cases handled by COs and medical doctors, there were no significant differences found. Therefore, the authors suggest that COs will continue to contribute to the healthcare system in Mali. However, Chilopora and colleagues also suggest that all COs should undertake surgical internships at the central hospital, and not district hospitals, to ensure equal competence.
Together, these studies and others suggest that with proper training, it is possible for foundation level doctors to perform emergency C-sections without the need for a specialist to be present. However, this is based on the assumption that they will perform such procedures under the supervision of consultants during their training programme. It is also important to note that these studies were carried out in a rural hospital setting, rather than a rural clinic, similar to the Maa clinic, where resources are limited. Also, the training programme lasted between 1-2 years, whereas the Maa training programme, provided by RCOG BD, will be an intensive course lasting only 6 months. Therefore, Maa doctors will not be performing emergency C-sections in the clinic. These cases will be referred to the tertiary hospital located a small distance away from the Maa clinic. It is encouraging that other countries have seen success in surgical task shifting. Although the pilot study of the HS model does not include secondary care services, Maa aims to integrate secondary care services into the HS model in the future.
Retention of specialised doctors
An important issue to tackle in the HS model is the retention of Maa specialised doctors and healthcare workers during their rotation in the rural Maa clinic. Absenteeism is a major problem which has hindered access to healthcare for hard to reach, rural populations in Bangladesh for many years. Darkwa and colleagues (2015) present qualitative data explaining why absenteeism occurs in the Sunamganj district. Table 2 summarises the major findings from this paper as to why specialist doctors are deterred from working in rural areas and how Maa aims to tackle these issues.
Table 2: Factors affecting doctor retention in rural villages and Maa’s proposed solutions.
Issues identified
Maa’s solution
Lack of career progression in rural areas.
The RCOG training programme will have different levels to complete and a separate certificate will be provided for successful completion of the courses. This will be indicative of career progression.
Lack of financial incentive – Bangladeshi doctors earn extra income through private practice in urban areas, this is not possible in rural areas.
Each doctor will only spend 3 months at the Maa clinic, after which they will return to their originalposts in hospitals and can treat private patients.
Difficult working conditions with intense shifts.
As mentioned above, doctors will only be required to complete a 9-5 shift, except the on-call doctor. The three doctors will work on a rota system to ensure the same doctor is not always on-call.
Also, their job is to act only as a primary healthcare provider. This is contrary to the job of doctors in the past, where they have been expected to provide primary, secondary and tertiary care during placements in rural areas.
Poor living conditions.
Maa will provide good living arrangements for doctors by partnering with businessmen who own hotels/accommodation in the local area.
The results of this study will provide an evaluation of whether the HS strategy to retain doctors is one which global health researchers should apply to other LMICs.
The importance of Skilled Birth Attendants
The Skilled Birth Attendants’ (SBAs) role in all studies thus far has been to assist in childbirth and to identify complications, leading to referral to a healthcare facility. SBAs are health professionals, such as midwives, doctors and nurses, who are trained to manage uncomplicated births and provide postnatal care. Encouraging the involvement of SBAs during home deliveries is a method by which maternal mortality and morbidity rates can be reduced. Based on this finding, the HS model aims to promote SBA use for high-risk mothers, by referring them to a hospital. Analysis of the BDHS report (NIPORT, 2014) by Bhowmik et. al. (2019), reveals that the SBA service rate in Bangladesh rose to 42% in 2014. However, this is still below the target of 50%, set by the government of Bangladesh. Also, data from Huq and colleagues (2015) suggests that the inclusion of SBAs in the model will increase the opportunity for underprivileged mothers to get appropriate care when needed the most.
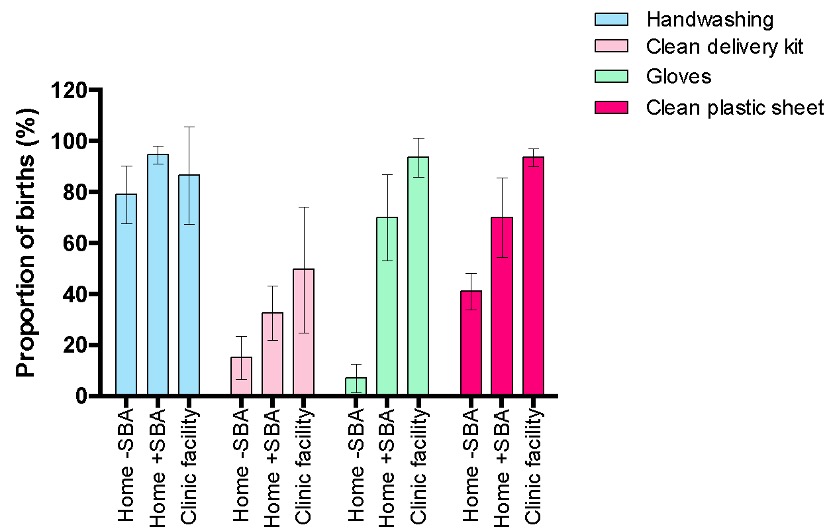
Specialised doctors should be able to act as SBAs in the future phases of the HS model, as there is evidence to suggest that the presence of SBAs greatly reduces maternal and neonatal mortality and morbidity rates. Pagel and colleagues (2014) compared essential newborn care (ENC) provisions found in rural health facilities and during home deliveries in the presence and absence of an SBA. Moulvibazaar, Bogra and Faridpur are the villages included in this study. In these villages, only 10% of pregnant women had facility births; 20% had home deliveries in the presence of an SBA and 70% had home deliveries without an SBA. Different antenatal hygienic care practices in the three Bangladeshi villages were compared. Figure 1 reveals that handwashing by birth attendants was high in all settings. Unfortunately, the proportion of births where a safe delivery kit was used was very low in all three settings. This may be for several reasons, for example, some clinics may have an autoclave system which cleans all instruments and resources used, making a kit unnecessary. Finally, the proportion of births where birth attendants wore gloves and used a clean plastic sheet for deliveries was higher in the presence of SBAs. Interestingly, the overall difference in percentage between the hygiene practices of SBAs during home deliveries and in clinic facilities is not large, suggesting that there is no major difference in the performance of safe antenatal practices between SBAs delivering at home and SBAs in hospitals. Therefore, Maa specialised doctors couldprovide care to the same standard as doctors and staff found in hospitals.
Despite having performed poorly in two of the ANC and PNC practices, Pagel and colleagues (2014) reveal that overall, Bangladesh is performing much better than other south-east Asian countries such as Nepal and India. Therefore, the aim of the HS model is to maintain high standards of care and improve the practices mentioned above.
Figure 1: Proportions of births receiving each antenatal hygienic care practice by delivery type with 95% confidence intervals. Adapted from Pagel et. al. (2014)
Community Skilled Birth Attendants programme
The CSBA programme was initiated by the Bangladeshi government, in collaboration with the WHO and UNFPA in 2003. The aim was to train community health workers, in an effort to reduce maternal mortality, by increasing the number of SBAs available in rural areas of Bangladesh. Those who were trained included welfare assistants (female paramedics), female health assistants and other community health workers who worked for the government, NGOs and private organisations. The midwifery training course lasted 6 months and covered basic skills, such as performing a normal delivery. CSBAs were also trained to recognise red flag symptoms in pregnancy, in order to refer mothers to nearby hospitals. Despite the success of the CSBA pilot study, the programme failed for several reasons (Turkmani et. al., 2015) (Table 2). Only 7,000 workers had been trained by 2015, which is less than half of the target initially proposed. Therefore, it was estimated that only 5% of the community would benefit from this intervention.
It is clear that there are some similarities between CSBAs and Maa specialised doctors. Both groups receive a 6-month training course to learn essential midwifery skills and their roles are also the same: perform normal/routine deliveries and recognise red flag symptoms to refer mothers to local hospitals. However, Maa has analysed the pitfalls of the CSBA programme and designed this study to successfully overcome them. The solutions are summarised in Table 2.
Table 2: A summary of the failures of the CSBA programme and Maa’s adaptations to tackle the problems.
CSBA failures
Maa’s solution/adaptation
The 6-month training course is too advanced for community health workers and trainers, leading to ineffective training. The language used in the course is too advanced for people with no medical knowledge. It is unclear who provided the training to these people.
Maa specialised doctors are of foundation level, thus literate and have medical knowledge. They can easily understand the content being taught. Training will be provided by RCOG BD who are specialists in maternal healthcare.
Some CSBAs were forced to attend training.
Maa specialised doctors willingly attend the 3-month rotation at the Maa clinic in order to complete the training course and receive a certificate from RCOGUK.
CSBAs had no financial incentive. They were paid the same salary but the workload was extremely high.
Maa specialised doctors are paid for their services during the 3 months at the Maa clinic. Doctors will work 9am-5pm shifts, hence workload is controlled.
Low acceptability at the community level.
Women’s groups and HBMs in the Hub-spokes model will raise awareness about the Maa clinic and its doctors, especially during ANCs. This allows familiarity with the organisation and building trust in the community.
CSBAs did not have a clearly defined role, leading to a lot of confusion and neglect from other healthcare providers in the local area.
The HS model has been planned very well and the roles of each individual team are well defined. All members of the model will be trained to understand their individual roles.
As mentioned above, Maa aims to integrate secondary health care services in future phases of the HS model but not the pilot study. Despite the evidence to suggest that doctors acting as SBAs will help reduce maternal mortality and morbidity, it is important to consider the safety of our patients first. In the current training programme, Maa doctors will not receive sufficient training to be able to attend births without a consultant being present to supervise them.
References:
Balsari, S., Simon, G. and Nair, R. (2017). Task shifting in health care: the risks of integrated medicine in India. The Lancet Global Health, 5(10), pp.e963-e964.
Bhowmik, J., Biswas, R. and Woldegiorgis, M. (2019). Antenatal care and skilled birth attendance in Bangladesh are influenced by female education and family affordability: BDHS 2014. Public Health, 170, pp.113-121.
Chilopora, G., Pereira, C. and Kamwendo, F. (2007). Postoperative outcome of caesarean sections and other major emergency obstetric surgery by clinical officers and medical officers in Malawi. Human Resources for Health, 5(1).
Darkwa, E., Newman, M. and Kawkab, M. (2015). A qualitative study of factors influencing retention of doctors and nurses at rural healthcare facilities in Bangladesh. BMC Health Services Research, 15(1).
de Jonge, E., Azad, K. and Hossen, M. (2018). Socioeconomic inequalities in newborn care during facility and home deliveries: a cross sectional analysis of data from demographic surveillance sites in rural Bangladesh, India and Nepal. International Journal for Equity in Health, 17(1).
Figueiredo, K., Gonçalves, G. and Batista, H. et. al., (2018). Actions of primary health care professionals to reduce maternal mortality in the Brazilian Northeast. International Journal for Equity in Health, 17(1).
National Institute of Population Research and Training (NIPORT), Mitra and Associates, and ICF International. 2015. Bangladesh Demographic and Health Survey 2014: Key Indicators. Dhaka, Bangladesh, and Rockville, Maryland, USA: NIPORT, Mitra and Associates, and ICF International.
Pembe, A., Carlstedt, A. and Urassa, D. et. al., (2010). Effectiveness of maternal referral system in a rural setting: a case study from Rufiji district, Tanzania. BMC Health Services Research, 10(1).
Smith, A., Shakespeare, J. and Dixon, A. (2019). [online] Kingsfund.org.uk. Available at: https://www.kingsfund.org.uk/sites/default/files/field/field_document/gps-maternity-care-gp-inquiry-research-paper-mar11.pdf [Accessed 1 Aug. 2019].
van Duinen, A., Kamara, M. and Hagander, L. et. al., (2019). Caesarean section performed by medical doctors and associate clinicians in Sierra Leone. BJS, 106(2), pp.e129-e137.
World Health Organisation (2012). WHO recommendations for the prevention and treatment of postpartum haemorrhage. ISBN 978 92 4 154850 2
World Health Organisation (2015). Pregnancy, Childbirth, Postpartum and Newborn Care: A guide for essential practice. ISBN: 9789241549356
Who.int. (2019). Primary health care. [online] Available at: https://www.who.int/news-room/fact-sheets/detail/primary-health-care [Accessed 8 Aug. 2019].
This website uses cookies to improve your experience. We'll assume you're ok with this, but you can opt-out if you wish. Cookie settingsACCEPT
Privacy & Cookies Policy
Privacy Overview
This website uses cookies to improve your experience while you navigate through the website. Out of these cookies, the cookies that are categorized as necessary are stored on your browser as they are essential for the working of basic functionalities of the website. We also use third-party cookies that help us analyze and understand how you use this website. These cookies will be stored in your browser only with your consent. You also have the option to opt-out of these cookies. But opting out of some of these cookies may have an effect on your browsing experience.
Necessary cookies are absolutely essential for the website to function properly. This category only includes cookies that ensures basic functionalities and security features of the website. These cookies do not store any personal information.
Any cookies that may not be particularly necessary for the website to function and is used specifically to collect user personal data via analytics, ads, other embedded contents are termed as non-necessary cookies. It is mandatory to procure user consent prior to running these cookies on your website.