Women’s groups are one such participatory community-based intervention, and they have been used as a tool to educate and empower communities in rural areas to improve maternal and neonatal health outcomes.
Since the Alma-Ata declaration in 1978, community participation has been recognised as an integral component to primary healthcare. Participatory community-based interventions are important in improving health outcomes, particularly amongst the poorest populations in developing countries (Rifkin, 1990; Rosato et al, 2008). They act as a capacity-building tool; empowering local populations to take responsibility for identifying and solving problems within their own communities (Morgan, 2001; Howard-Grabman and Snetro, 2003; Manandhar et al., 2004; Nair et al., 2012). Paolo Freire highlighted that sustainable change will only occur if poor communities are engaged in dialogue and collectively decide to act to improve their own health and development problems (Freire, 1970).
Women’s groups are one such participatory community-based intervention, and they have been used as a tool to educate and empower communities in rural areas to improve maternal and neonatal health outcomes. They provide the opportunity for local women and other members of the community to convene regularly to identify problems in the community and exchange ideas on how to tackle them. The purpose of this report is to highlight the successes and failures of these women’s groups and describe how the Maternal Aid Association (Maa) will use this evidence to establish effective and sustainable women’s groups in rural Bangladesh. Women’s groups have proven to be a low-cost yet highly effective approach to reducing maternal and neonatal mortality in resource-poor settings (Prost et al, 2013). Maa aims to incorporate these women’s groups into rural Bangladesh as a small yet integral part of its Hub-spokes model.
STUDY METHODS
Several studies of women’s groups have been conducted in rural Bangladesh, in the districts Bogra, Moulvibazar, and Faridpur, (Azad et al, 2010; Fottrell et al, 2013), as well as in India (Tripathy et al, 2010), Nepal (Manandhar et al, 2004) and Malawi (Lewycka et al, 2013). Whilst the details of each approach vary, the overarching method was the same.
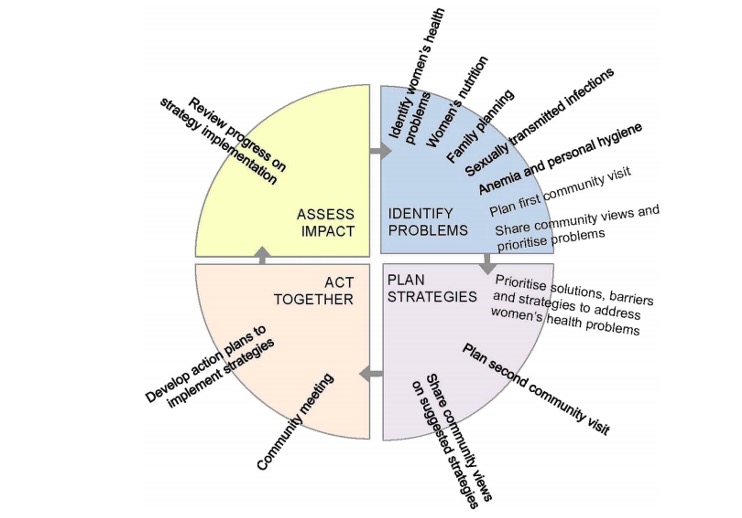
The women’s groups were led by facilitators. Facilitators were locally recruited, literate women who undertook 5-11 days of training to qualify them to conduct between 10-18 monthly women’s groups in different rural areas. Facilitators may have received refresher training, which in some cases were every four months (Lewyka et al, 2013). They became educated on maternal and neonatal health problems relevant to that area and guided group discussions in the women’s group, using picture cards, story-telling and role-playing as tools to engage members (Manadhar et al, 2004, Tripathy et al, 2010). Facilitators were trained to adopt the Participatory Learning and Action (PLA) cycle to empower groups to identify and tackle problems. This approach encourages women to identify maternal and neonatal health problems, plan strategies to tackle them, implement these strategies and finally, assess their impact (Figure 1).
Figure 1. Participatory Learning and Action cycle (Harris-Fry et al, 2016)
The women’s groups were open to all members of the community, including the elderly, children and men who often took a more passive role. However, the target population was women of reproductive age. These women could opt to commit to more responsibility, such as organising group meetings and implementing the strategies decided upon. Previous strategies that were implemented in Nepal include the generation of emergency maternal and child health funds, production and management of stretchers, local production and distribution of clean delivery kits, home visits by group members to newly pregnant mothers, and raising awareness through plays and locally made films (Manandhar et al, 2004; Morrison et al, 2005).
To ensure the programme ran smoothly and facilitators were well supported, each facilitator had a supervisor whose role was to obtain permission and support from community and religious leaders and observe occasional sessions in order to provide constructive feedback for facilitators. The ratios of supervisors to facilitators differed between the studies. For example, there was one supervisor to three facilitators in Nepal (Manandhar et al, 2004), and one supervisor to six facilitators in Malawi (Lewycka et al, 2013).
In all the trials, the women’s groups were supplemented with basic healthcare strengthening in that area. For example, in Malawi, health workers from every facility were trained in essential newborn care, lifesaving skills, and safe motherhood, and the facilities were provided equipment such as bulb syringes, resuscitation tables, ambu-bags and cord clamps (Lewycka et al, 2013).
The studies explored the problems they experienced during the implementation of the women’s groups. Common problems included poor retainment of facilitators over the trial period and postponement of meetings due to adverse climate conditions as facilitators could not access certain areas (Azad et al, 2010), as well as delays due to religious holidays, harvest commitments, and flooding (Fottrell et al, 2013). It is also important to note the socio-economic, environmental and cultural context these women’s groups are established in, as these may play a key role in inhibiting access to healthcare (Azad et al, 2010; Morrison et al, 2010; Harris-Fry et al, 2016). For example, there was evidence of gender-based barriers that prevented women from joining the groups, seeking healthcare, and implementing strategies the group had decided upon (Azad et al, 2010). Maa will take these problems into consideration when developing a strategy to establish women’s groups in Bangladesh.
Primary study outcomes: neonatal mortality rate, maternal mortality rate and stillbirth rates
The primary outcome for all the studies conducted was the neonatal mortality ratio (NMR), followed by maternal mortality ratio (MMR) and stillbirth rates. The NMR was significantly reduced in clusters with women’s groups compared to control clusters in Nepal (Manandhar et al, 2004), Bangladesh (Fottrell et al, 2013), Malawi, (Lewycka et al, 2013) and India by 30%, 38% and 41% and 45% respectively. Only one study showed women’s groups to have no significant impact on neonatal mortality in rural Bangladesh (Azad et al, 2010). This was later understood to be a result of inadequate population coverage, and once the coverage improved from 1 group per 1414 population to 1 group per 309 population, the NMR was significantly reduced by 38% (Fottrell et al, 2013).
In terms of the MMR, Azad et al (2010) noted no significant difference in Bangladesh, and in fact, stated that maternal mortality was generally higher in intervention areas than control areas. However, as the MMR was not always the primary outcome, many studies were not powered to measure the MMR. Consequently, the study in Bangladesh by Fottrell et al (2013) did not comment on it, making it unclear whether improving population coverage in Bangladesh is correlated with improved MMR. Other studies (India and Nepal) mentioned a reduction in MMR but highlighted the need for the study to be repeated as it was underpowered, and therefore the MMR was not reliable. For example, there was a reduction in MMR in India by 20% in intervention areas after 3 years (Tripathy et al, 2010), and in Nepal, MMR was reduced by 80% (Manandhar et al, 2004). On the other hand, the study in Malawi was powered to measure the MMR and observed a significant 74% reduction (Lewycka et al, 2013). Unfortunately, the women’s groups had no significant impact on stillbirth rates (Fottrell et al, 2013; Manandhar et al, 2004; Prost et al, 2013).
This data is encouraging for Maa as it demonstrates how effective women’s groups can be in impacting health outcomes, particularly the NMR, as long as there is adequate population coverage. It appears that the MMR can be significantly reduced through these women’s groups, but the evidence in this area is limited. The HS model aims to fill the gap in evidence regarding MMR in Bangladesh in future studies.
Secondary study outcomes: health indicators
Secondary outcomes such as changes in health education and awareness, safe and hygienic deliveries, early neonatal care, and health-seeking behaviours and utilisation of health facilities were also measured. Whilst the women’s groups themselves identified and explored a range of topics they deemed relevant, key educational messages were delivered by all facilitators. Such topics included but were not limited to a) having a safe delivery, b) early neonatal care, and c) encouraging health-seeking behaviours.
The studies show that women’s groups have significantly improved the number of safe deliveries. In Nepal (Manandhar et al, 2004), India (Tripathy et al, 2010), Malawi (Lewycka et al, 2013) and Bangladesh (Fottrell et al, 2013), women’s groups led to increased use of safe home delivery kits, with birth attendants more likely to wash their hands and boil the thread to tie the umbilical cord in India and Nepal.
The studies by Azad et al, (2010), Fottrell et al (2013) and Lewycka et al (2013) further show that women’s groups have significantly improved early newborn care practices such as early wrapping of the newborn, avoidance of early bathing, and early and exclusive breastfeeding for up to 6 weeks. Improvements in early and exclusive breastfeeding for up to 6 weeks were also noted in India (Tripathy et al, 2010) and in Nepal, this was for up to 6 months (Manandhar et al, 2004). There were also significant improvements in the number of newborn immunisations in Nepal compared to control clusters.
With regards to encouraging health-seeking behaviours, in Nepal, there were more women having institutional deliveries, receiving antenatal care, and seeking care for themselves and their newborns in the event of illness in intervention clusters (Manandhar et al, 2004). There were also fewer infection-related deaths in intervention clusters in Nepal (Manandhar et al, 2004). These health-seeking improvements were also noted in Malawi though the indicators were less conclusive (Lewycka et al, 2013). On the other hand, in Bangladesh, the proportion of institutional deliveries was slightly higher in control clusters than intervention clusters (Azad et al, 2010), and even when this study was scaled up, health service utilisation did not significantly increase in areas with women’s groups (Fottrell et al, 2013). Similarly, in India, there was no significant difference in health-seeking behaviours between control and intervention clusters (Tripathy et al, 2010). This is concerning as Maa aims for women’s groups to encourage positive health-seeking behaviours, such as attending antenatal and postnatal checkups. The low uptake of health services despite the implementation of women’s groups may be because there is no evidence of these women’s groups being formally linked to the healthcare system. This suggests that if women’s groups are integrated within the wider healthcare system, women may be able to act on the knowledge they have gained with ease, which may lead to a significant increase in health service utilisation in the population. Maa aims to target this by seamlessly integrating women’s groups within its wider HS model. Additionally, Harris-Fry et al (2016) suggests that women’s groups may appear to be more effective in changing health-promoting knowledge, rather than influencing health-seeking behaviours, due to a time lag; any changes in attitudes and behaviours may take longer to come into effect than changes in knowledge, and the trials may not have been conducted for long enough to observe this.
Study outcomes: conclusion
Together, this evidence suggests a strong association between establishing women’s groups and observing improved maternal and neonatal health outcomes in rural areas. Whilst MMR cannot confidently be commented on due to the lack of statistical evidence, and stillbirth rates showing no improvement, the impact on NMR alone makes women’s groups cost-effective (Prost et al, 2013). Cost-effectiveness was expressed as the incremental cost per neonatal death averted and life-year saved. According to a meta-analysis conducted by Prost et al (2013) that analysed seven studies that conducted similar women’s groups in low-resource settings (including all five that were explored in this report), the intervention is highly cost-effective by WHO standards and could save an estimated 283,000 newborn infants and 36,600 mothers per year if implemented in rural areas of 74 Countdown countries.
Beyond health outcomes, in areas with women’s groups, women were more informed on health complications, undertook more positive health practices and in some areas, had improved health-seeking behaviours. It is on the basis of this evidence that Maa aims to establish women’s groups in rural Bangladesh, piloting in Moulvibazar in 2020. Maa will use these studies as a source of guidance but understands the importance of identifying and learning from any problems they experienced in order to establish the most effective women’s groups.
Maa’s women’s groups
Maa aims to revolutionise the delivery of maternal healthcare in Bangladesh through the HS model. The model aims to provide specialised doctors working in a primary care centre (the Maa clinic), where they will deliver antenatal care for high-risk pregnancies, identify and confirm any red-flag symptoms, and refer patients to nearby tertiary hospitals when necessary. The model also includes Health Brigade Members (HBMs) who are the link between the rural community and primary health services. They will be working with the women’s groups to identify pregnant women and new mothers in the community and offer full antenatal and postnatal care to them, respectively. They will screen mothers for red-flag signs and symptoms, record the results on the MaaConnect app, identify high-risk pregnancies and refer them to the Maa clinic as appropriate via the app. They will also provide basic preventative care to women in more remote areas, as well as comprehensive one-to-one education.
However, to maximise the impact of this healthcare and education, Maa needs to ensure the community are receptive towards it. Rural communities in Bangladesh need to be educated on when and how to seek care and have the means to do so when they need it. By fostering an environment of trust and empowerment within these women’s groups, women may be more likely to engage with health workers and services during pregnancy. This will, therefore, provide a convenient point of access for HBMs to find pregnant women who may benefit from simple health checks and education.
Therefore, community participation, which in this case will be through women’s groups is essential in generating a good relationship between primary services and their users. This differentiates Maa’s women’s groups from previous studies where the women’s groups were supplemented with basic healthcare strengthening but were not formally linked to the healthcare system. This may have been the reason why some studies did not observe asignificant increase in health service utilisation despite the presence of women’s groups (Azad et al, 2010; Tripathy et al, 2010; Fottrell et al, 2013). Maa aims to integrate women’s groups within the wider healthcare system and observe whether this positively influences health-seeking behaviours and practices.
With the support of Dr Edward Fottrell and Professor Kishwar Azad, Maa is hoping to reintroduce women’s groups to rural Bangladesh using an approach similar to the one conducted in Bangladesh by Fottrell et al (2013) as a key community component to its HS model.
Maa’s women’s groups will aim to have a population coverage of one facilitator for every 300-400 population, as this was the ratio that proved most effective in all of the studies explored, and Azad et al (2010) highlighted the significance of population coverage in achieving better health outcomes. The women’s group meetings will occur fortnightly instead of monthly as all previous studies have done, as Maa aims to observe whether more regular sessions have a greater impact. From the evidence, there would be an expected attendance of 15-20 members per meeting. The location of the meetings should be public and easily accessible; preferably in an open outdoor space, however, this will vary between sites and depend on climate conditions.
The topics of the meetings will be determined by the groups, however, facilitators will help guide the group to a decision. Maa does not want to be prescriptive and impose predetermined topics that Maa believes to be most important for the communities. Having said this, Maa recognises that a key problem from previous trials was that the socio-cultural, economic and infrastructural context cannot be undermined, as it impacts whether or not women can join the groups and access healthcare. If these are not addressed, then the potential impact of these groups will be reduced. Therefore, Maa would encourage women’s groups to discuss and explore solutions to these other determinants of health and would support the implementation of these strategies.
The key roles Maa have identified within the women’s groups include the facilitator, the group members, and supervisors. Maa also aims to conduct its own research trial and therefore will have a team of researchers from the Maa Bangladesh team and the Maa UK Academics and Innovations team.
Facilitators
Facilitators will lead the group meetings, and each facilitator will be responsible for 14 meetings per month. The criteria for employing facilitators will be that they are local, literate women who have at minimum a high school education. They will undergo a training course for one week led by a senior facilitator in Sylhet. This training will include maternal and neonatal health education, covering topics such as: having a healthy pregnancy, nutrition, sexual and reproductive health, hygiene, having a safe delivery, and newborn care. Facilitators will learn how to guide discussions using the Participatory Learning and Action cycle and ensure engagement from group members. The training will also demonstrate how to guide discussions and plan strategies for problems that are sensitive in nature, such as overcoming unhelpful cultural or gender-based expectations or navigating difficult socio-economic conditions in order to receive care.
Facilitators will have a facilitation manual to revise their training, and they will also be equipped with materials such as flipcharts, cards and leaflets in order to deliver the sessions in a dynamic and engaging way. For the purpose of continuity, the facilitators will remain in the same areas for every session, to allow them to develop strong relationships with the women and the communities.
To retain facilitators, they will be given a comfortable salary by Maa; of up to 10,000 taka per month. They will also receive support from supervisors to ensure they are fully prepared and equipped. Facilitators may, therefore, be provided with bicycles, umbrellas and walking boots in order to access more areas. This will hopefully allow sessions to remain consistent and avoid the postponing of too many sessions. However, the safety of facilitators is always paramount, and Maa would advise against accessing environmentally hazardous areas. Maa may also provide them with certification and opportunities for progression if they wish.
Group members
The women’s groups main target audience is women of reproductive age (15-49), particularly newly pregnant women. The women’s groups will consist of ‘active members’ and ‘community members.’ Active membership will only be open to local women of reproductive age, who must commit to more responsibilities such as organising group meetings and activities, actively planning and implementing strategies the groups decide upon and continue community engagement between sessions. Community membership will be open to all other women, as well as men, young children and the elderly, who can attend sessions and take a more passive role. Further community engagement will occur between active group members and community and religious leaders, local school teachers, health workers etc., through monthly community meetings. This will allow women to discuss key health problems identified and prioritised within the women’s groups and share their proposed action plans. In doing so, women can receive feedback and obtain approval and support in implementing their plans.
Supervisors
Finally, women’s groups will be overseen by supervisors. They will be locally recruited women with a college-level education who have a comprehensive understanding of the women’s groups aims and approach. Their role includes liaising with and delivering presentations to community leaders, as well as government and non-government healthcare professionals to foster a supportive environment for the women’s groups. They must also ensure the quality of women’s groups is maintained and provide support to facilitators. To do this, supervisors will visit each facilitator fortnightly, and observe at least one of their meetings. This will allow them to respond to any concerns the facilitators may have and ensure they are comfortable. They will also have the opportunity to offer feedback on increasing the effectiveness of the meetings. Finally, they can provide or recommend further training for the facilitator, and provide additional material, practical or emotional support and advice. This is an essential role for Maa as an inability to retain and adequately support facilitators has been a recurrent theme in previous studies.
Maa will be conducting a pilot study for the women’s groups in 2020 in 7 rural villages in Moulvibazar. Each village will have fortnightly women’s groups, and these will be led by one facilitator. Thus, the facilitator will be leading 14 sessions per month and will be paid 10,000 taka. They will be fully equipped and supported by a supervisor.
CONCLUSION
This report explores the evidence behind women’s group trials that have been conducted in rural, resource-poor settings over the past 20 years. It outlines their successes and failures, and the problems they experienced in implementing their programmes. These studies will pave the way for Maa to establish women’s groups in rural Bangladesh, which will also follow a PLA approach. The key changes Maa will make to previous models to hopefully improve the effectiveness of women’s groups is to a) deliver fortnightly women’s groups instead of monthly, and b) integrate women’s groups into the wider healthcare system (Hub-spokes model) by providing direct access to HBMs and subsequently, primary care facilities. Unlike previous studies, Maa will also have a stronger emphasis on MMR as a primary outcome, as opposed to NMR, and may consequently contribute significantly to the literature in this area. Maa aims for these groups to continue long-term, as they have proven to be a sustainable, cost-effective and beneficial way of engaging, educating and empowering communities to improve the state of maternal and neonatal health. These women’s groups will complement and reiterate the work of HBMs, and form an essential community component to the Hub-spokes model.
REFERENCES
Azad, K., Barnett, S., Banerjee, B., (2010) Effect of scaling up women’s groups on birth outcomes in three rural districts in Bangladesh: a cluster-randomised controlled trial. Lancet, 375: 1193-202
Fottrell, E., Azad, K., Kuddus, A., et al. (2013) The effect of increased coverage of participatory women’s groups on neonatal mortality in Bangladesh – a cluster randomised trial. JAMA pediatrics, 167(9)
Freire, P. (1970) Pedagogy of the oppressed, Penguin Books, London, UK.
Harris-Fry, H., Azad, K., Younes, L., (2016) Formative evaluation of a participatory women’s group intervention to improve reproductive and women’s health outcomes in rural Bangladesh: a controlled before and after study. J Epidemiol Community Health, 70(7):663-70
Howard-Grabman, L. and Snetro, G. (2003) How to mobilize communities for health and social change, Johns Hopkins Bloomberg School of Public Health, Baltimore, United States of America.
Lewycka S, Mwansambo C, Rosato M, et al. (2013) Effect of women’s groups and volunteer peer counselling on rates of mortality, morbidity, and health behaviours in mothers and children in rural Malawi (MaiMwana): a factorial, cluster randomised controlled trial. Lancet, 381: 1721–35.
Manandhar, D. S., Osrin, D., Shrestha, B. P., et al. (2004) Effect of participatory intervention with women’s groups on birth outcomes in Nepal: cluster-randomised controlled trial, Lancet, 364, 970–979.
Morgan, L. M. (2001) Community participation in health: perpetual allure, persistent challenge, Health Policy and Planning, 16 (3), 221–230.
Morrison J, Thapa R, Hartley S, et al. (2010) How women’s groups improve maternal and newborn health in Makwanpur, Nepal: a qualitative study. Int Health, 2: 25–35.
Nair, N., Tripathy, P., Costello, A., et al. (2012) Mobilizing women’s groups for improved maternal and newborn health: evidence for impact and challenges for sustainability and scale up, International Journal of Gynaecology and Obstetrics, 199, S22–S25.
Prost, A., Colbourn, T., Seward, N., et al. (2013) Women’s groups practising participatory learning and action to improve maternal and newborn health in low resource settings: a systematic and meta-analysis, Lancet, 381, 1736–1746.
Rifkin, S. B. (1990) Community participation in maternal and child health family planning programmes: an analysis based on case study materials, World Health Organization, Geneva, Switzerland.
Rosato, M., Laverack, G., Grabman, L. H., et al. (2008) Community participation: lessons for maternal, newborn and child health, Lancet, 372, 962–971.
Tripathy, P., Nair, N., Barnett, S., et al. (2010) Effect of a participatory intervention with women’s groups on birth outcomes and maternal depression in Jharkhand and Orissa, India: a cluster-randomised controlled trial. Lancet, 375: 1182–92
World Health Organization. (2014) WHO recommendation on community mobilization through facilitated participatory learning and action cycles with women’s groups for maternal and newborn health, World Health Organization, Geneva.
This website uses cookies to improve your experience. We'll assume you're ok with this, but you can opt-out if you wish. Cookie settingsACCEPT
Privacy & Cookies Policy
Privacy Overview
This website uses cookies to improve your experience while you navigate through the website. Out of these cookies, the cookies that are categorized as necessary are stored on your browser as they are essential for the working of basic functionalities of the website. We also use third-party cookies that help us analyze and understand how you use this website. These cookies will be stored in your browser only with your consent. You also have the option to opt-out of these cookies. But opting out of some of these cookies may have an effect on your browsing experience.
Necessary cookies are absolutely essential for the website to function properly. This category only includes cookies that ensures basic functionalities and security features of the website. These cookies do not store any personal information.
Any cookies that may not be particularly necessary for the website to function and is used specifically to collect user personal data via analytics, ads, other embedded contents are termed as non-necessary cookies. It is mandatory to procure user consent prior to running these cookies on your website.